
To understand a passage in today’s page of Talmud requires a deep dive into lunar mechanics. Take it slowly and it all makes sense. We will get back to the Talmud in a moment. But first, some astronomy.
The Molad and the lunar conjunction
Each Jewish lunar cycle begins on the molad (lit. birth). This is the moment at which the sun, the moon and the earth line up. At that time the moon is completely invisible because no sunlight can reach the side of the moon that faces us. In astronomy, this moment is called the lunar conjunction.

The precise moment of the lunar conjunction. It should be the same as the calculated time of the molad. But it isn’t.
The Jewish lunar month (based on Babylonian measurements) has a fixed period of 29 days, 12 hours, 44 minutes and 3+1/3 second (or 29 days, 12 hours, and 793 chalakim, a chelek being 1/1080 of an hour). So if you know the time of the molad of one Jewish month, the next one will be precisely 29 days, 12 hours, 44 minutes and 31/3 seconds later. On the Shabbat before the start of every Jewish month (except one), the time of the molad is announced in the synagogue. The first day of that new month follows the molad, though the interval of time between the two varies. So far so good.
Here’s the Problem - and you could even see it

From here.
The problem is that the length of the calculated molad and the actual length of time between one conjunction and the next is not the same. There was a visual demonstration of this in North America during the total solar eclipse of 2017.
A total solar eclipse occurs when the moon gets directly between the sun and the earth and they are all on the same plane. That time is of course by definition, the same as the lunar conjunction for that month. The 2017 eclipse began on August 21 at 15:46 GMT which was 5:58pm in Jerusalem. That was when the moon started to move across the face of the sun. The total eclipse - when the moon directly covered the sun, occurred at 18:25 and 35 seconds GMT, which was 8:25:35pm in Jerusalem. That is the true astronomic lunar conjunction. But the molad for that month (which was Rosh Chodesh Elul) was announced as “Tuesday, August 22, at 10:44 a.m. and 15 chalakim” (Jerusalem time) — about 12 hours and 20 minutes hours later.
That solar eclipse (which I was lucky enough to witness on the beach in Charleston South Carolina - it was amazing-) visibly demonstrated two things. First, that molad we announce on the Shabbat preceding Rosh Chodesh represents a theoretical time only, and has absolutely no relationship to any astronomical phenomenon. And second, that the molad and the lunar conjunction are often several hours apart.
Why the molad time is not astronomically correct
The length of the Jewish lunar month is very precise, but alas, not accurate. Or at least not accurate enough. This is because the actual length of a lunar month varies from month to month and from year to year. It is affected by the speed of the earth’s orbit around the sun which changes as the earth gets closer or further away from the sun, and the changing distance of the moon from the earth (neither orbit being perfectly circular). NASA kindly provided a histogram which shows the length of the lunar month over 5,000 years. As you can see, thousands and thousands of lunar months have longer or shorter lengths compared to the mean length of the month.

The actual lunar month is longer than the molad month when the earth is moving at its slowest (the aphelion) and the moon is moving at its fastest (the perigee). In addition, the average length of our solar day (fixed at 24 hours) is getting longer as the tides imperceptibly slow the spin of the earth on its axis. The moon also slows the spin of the earth; every 100 years the day is about 2 milliseconds longer.
Today the average difference between the traditional moladot and the true mean lunar conjunctions, (referred to the meridian of Jerusalem) range from 2+1/2 hours early (Nisan) to 5 +2/3 hours late (Tishrei, Cheshvan), but the maximum differences range from 12 hours early to 16 hours late.
Sometimes then, the Jewish lunar month is shorter or longer than the actual lunar month, but over time it is not all averaging out. Something remarkable is happening: more and more of the calculated molad lunar months are falling behind the actual new moon. You can see this graphically below, thanks to the clever work of Dr. Irv Bromberg at the university of Toronto. The chart depicts the average relationship between the molad and the actual time of the lunar conjunction. The difference between the red line and the blue curve represents the error of the molad with respect to the actual lunar conjunction.
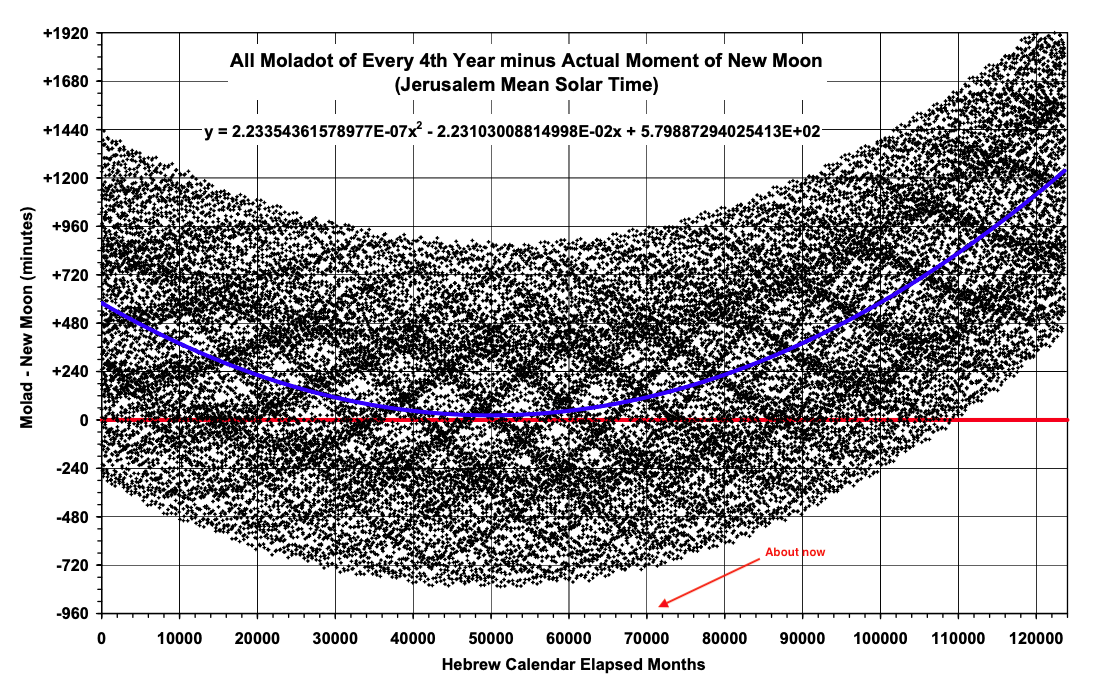
Dots above the thick horizontal line at zero indicate months in which the molad was or will be after the actual new moon. Dots below the thick horizontal line at zero indicate months in which the molad was or will be before the actual new moon.The difference between the red line and the blue curve represents the error of the molad with respect to the actual lunar conjunction. From here.
Now we can tackle today’s daf
Since some Jewish months have 29 days and others have 30, the average should be 29 1/2 days, But what do we do with that extra 44m and 3secs (or 793 chalakim) left over each month? Eventually they will add up to an entire 24-hour day, and so every three years or so an additional day must be added into the length of one of the Jewish months to bring it back into synchrony with the true lunar conjunction. In such a Jewish year (if it is a regular year) there will then be 355 days instead of the usual 354.
But even this adjustment is not enough. This three-year tweek still leaves an additional 48 minutes each year which adds up to just over one day every 30 years.* So every 30 years an additional day must be added to one of the Jewish months, and (if it is a regular year) there will then be 355 days instead of the usual 354.
ערכין ט,ב
והאיכא יומא דשעי ויומא דתלתין שני
This extra fraction beyond twenty-nine and a half days is compounded month after month and year after year, and as a result, eventually there is an additional day that must be added to the calendar every three years due to the accumulation of hours, and an additional day that must be added every thirty years due to a further accumulation of the extra parts of an hour.
But as we have seen even this fix does not get us back on track over the long run. In about another 3,000 years every calculated molad will be after the actual lunar conjunction, and the difference will grow over time (following the path of the blue curve in the graph above). Who will fix the problem then?
“ואין לנו לדאוג כ”כ יותר כי בודאי בעת ההיא וגם הרבה קודם יהיה הגאולה ונקדש ע”פ הראיה
There is no need to worry [about any future problems with the calendar] for certainly by that time the Redemption will have occurred and we will go back to sanctifying the new moon through the testimony of witnesses. ”
*For the calendrically inclined:
1 Jewish lunar month= 29d 12 h 793ch
Those extra 793ch are a problem.
Over a year of 12m they add (793ch x 12=) 9,516ch or 8h 48s to the length of the lunar cycle.
So over 3 years that is an additional 24 hours = 1 day PLUS 876 ch or 48m 40 secs
Over 30 years that additional 876ch is 26,280ch or just over one day (one day is 25,920ch).






